
By: Jessica S. Roller
In the United States, heart disease is the leading cause of death for men and women across most racial and ethnic groups. About 659,000 people in the United States die from heart disease each year, or about 1 in every 4 deaths, costing the United States about $363 billion per year.1-2 Often symptoms of heart disease go unnoticed by patients until the patient experiences a major cardiovascular event, such as a heart attack or stroke.2-3 But this doesn’t have to be the case; several modifiable risk factors for heart disease are known, including:
- High blood pressure
- High blood cholesterol
- Smoking
- Diabetes
- Obesity/ being overweight
- Physical inactivity
- Unhealthy diet
The first step in addressing risk factors is to identify them through routine health screenings. It is recommended that all patients between the ages of 40 and 75 be screened regularly for their risk of cardiovascular disease (CVD).3 Patients at moderate to high risk for major cardiovascular events can reduce their risk through interventions such as lifestyle modification, smoking cessation, and medication. Being the most accessible healthcare professional, community-based pharmacists have an opportunity to identify patients at risk, intervene, and provide ongoing support to these patients through education and medication management.
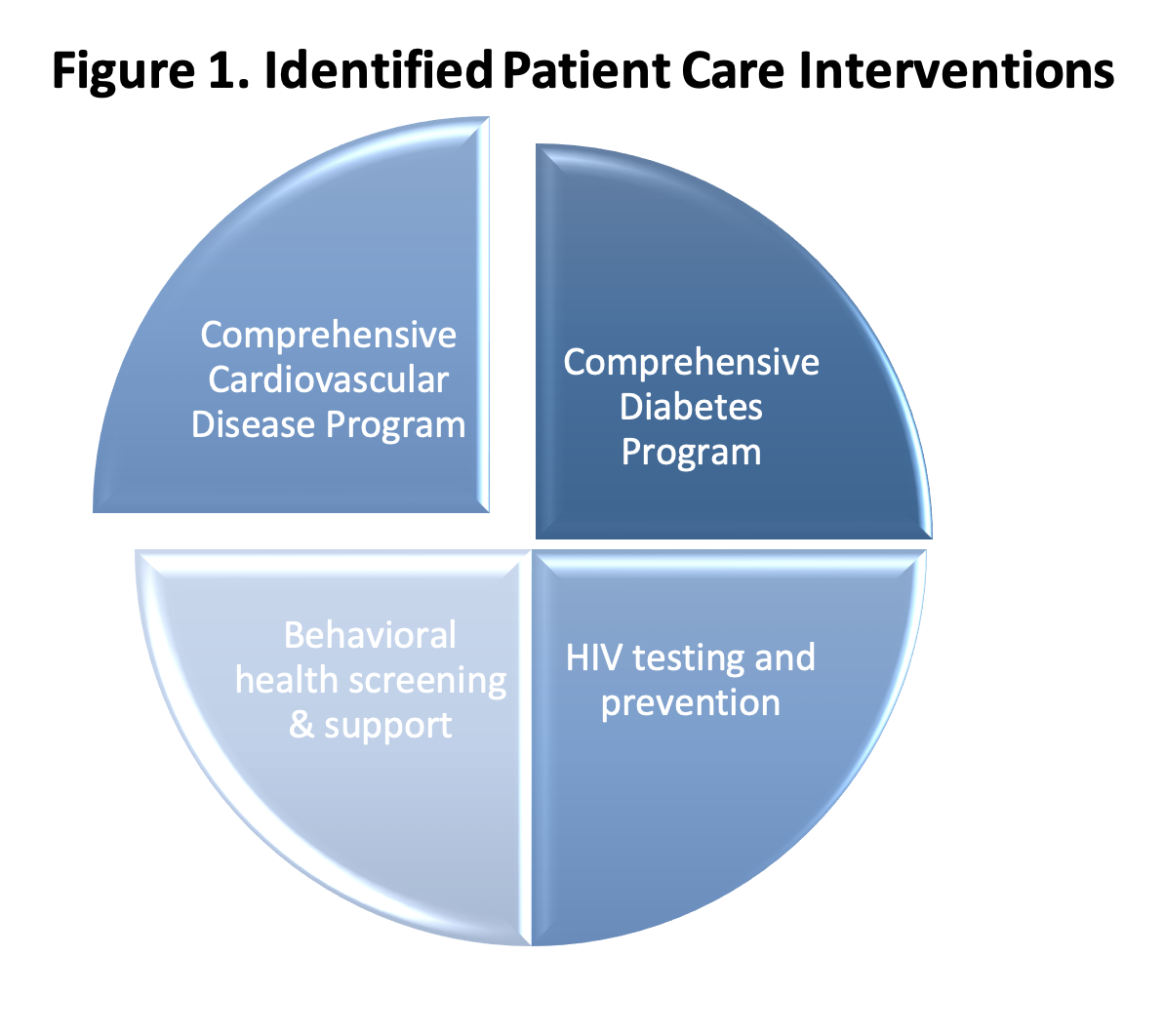
To support the expansion of patient access to community-based healthcare interventions addressing heart disease, the University of North Carolina Eshelman School of Pharmacy has partnered with the National Association of Chain Drug Stores (NACDS) Foundation to identify and create innovative community pharmacy care delivery models targeting chronic disease states, including cardiovascular disease. The project, titled Community-based Value-driven Care Initiative (CVCI), explores the feasibility and effectiveness of four patient-centered, quality-driven care interventions to advance population health (see Figure 1). These interventions are being implemented across diverse community pharmacy organizations to evaluate their feasibility, sustainability, and potential impact on population health.
The cardiovascular intervention is split into two programs: 1) A screening & referral (S&R) program and 2) A full CVD program consisting of medication management and health education (see Figure 2). The overall goal for the CVD screening and referral program is to increase access to CVD care for adults and to identify patients at risk for CVD with referral for diagnosis by a physician. The overall goal for the full CVD program is to optimize treatment through provision of evidence-based medication management and health education practices over a 6-month period.

To support sustainability of the CVD intervention over time, the UNC team has also established an Expert Stakeholder Group (ESG). The purpose of the ESG is to better understand patient health needs and align those needs with feasible community pharmacy interventions to facilitate a pathway towards sustainability.The cardiovascular intervention is currently being implemented by three community pharmacy organizations. The first organization is part of a regional supermarket chain with over 100 pharmacies in the Mid-Atlantic region. Two locations are participating and will be adding the CVD intervention to their other patient care services which include point-of-care testing, diabetes education, and immunizations. The second organization is an independent pharmacy group located in the Midwest; the two participating locations currently offer individualized patient care, medication counseling, and immunizations for their communities. The third organization, an independent pharmacy franchise located in the Midwest, is known for providing health screenings, immunizations, and diabetes education services. Five pharmacies from this organization will be participating in the project. All participating pharmacies had begun patient recruitment by the end of April 2022.
Interested in learning more about the project?
Come back here to check out future blogs and follow us on Twitter @unc_pace for updates. Read more about the project here.
Jessica S. Roller, PharmD is a Practice Advancement Fellow at the UNC Eshelman School of Pharmacy.
References:
- CDC – Heart Disease – Heart Disease Statistics and Maps. https://www.cdc.gov/heartdisease/facts.htm. March 29, 2022.
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation. 2021 Feb 23;143(8):e254-e743.
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019 Sep 10;140(11):e596-e646.
One Response to “Cardiovascular disease management in community-based pharmacies: How pharmacists can make a difference”
Vik
We at Drug Mart Pharmacy in South Plainfield, NJ used this article to discuss with our entire staff about the the role we can play in making a difference for patients in our community pharmacy. We already strive to keep patients compliant through Medication Therapy Management using Outcomes and Equipp. This provided more information on what we can do to take our care to the next level.